As of May 9, 2021, about 0.6 billion people around the world had been vaccinated with at least one dose of COVID-19 vaccines, accounting for about 7.8% of the world's population . This mass vaccination should allow for the identification of more uncommon and rare AEFI. According to the Vaccine Adverse Event Reporting System and V-safe system of the US Centers for Disease Control and Prevention , the rates of non-serious AEFI after public administration of BNT162b2 and mRNA-1273 were similar to the clinical trials. Variations in the incidence of anaphylaxis between countries are to be expected, as the numbers vaccinated in most countries to date are relatively small compared with the USA, and the reporting rates of AEFI from passive surveillance are biased. A causal link of thrombosis and thrombocytopenia with adenoviral vector vaccines (ChAdOx1 nCoV-19 and Ad26.COV2.S) was noted after mass public vaccination, including several deaths and severe outcomes . While rare side effects should not derail vaccination efforts , a thorough risk-benefit analysis is required.

Several studies have explored the safety profile of two mRNA vaccines (BNT162b2 and mRNA-1273) in HIV-positive populations , immunosuppressive patients , and pregnant women , revealing no evidence of unexpected serious adverse events. Further evaluation of the benefit-risk profile is warranted in these specific populations. The most common adverse reactions in clinical trial were typically mild fatigue and headache .

Rare myocarditis and pericarditis, mostly in male adolescents and young adults . About 1 in 6 recipients reported adverse reactions after 2nd dose in clinical trial, especially fatigue or muscle pain . About 1 in 130,000 recipients required hospitalization for Guillain Barré syndrome, a neurological disorder in which the body's immune system damages nerve cells, causing muscle weakness and sometimes paralysis. Vaccine recipients did not report serious adverse reactions more often than placebo recipients.
Mild to moderate reactions included soreness, headache, fatigue, muscle pain. Most common adverse reactions in clinical trials were flu-like illness, injection-site reactions, headache, and asthenia . Vaccine recipients did not report serious adverse events more frequently than placebo recipients .

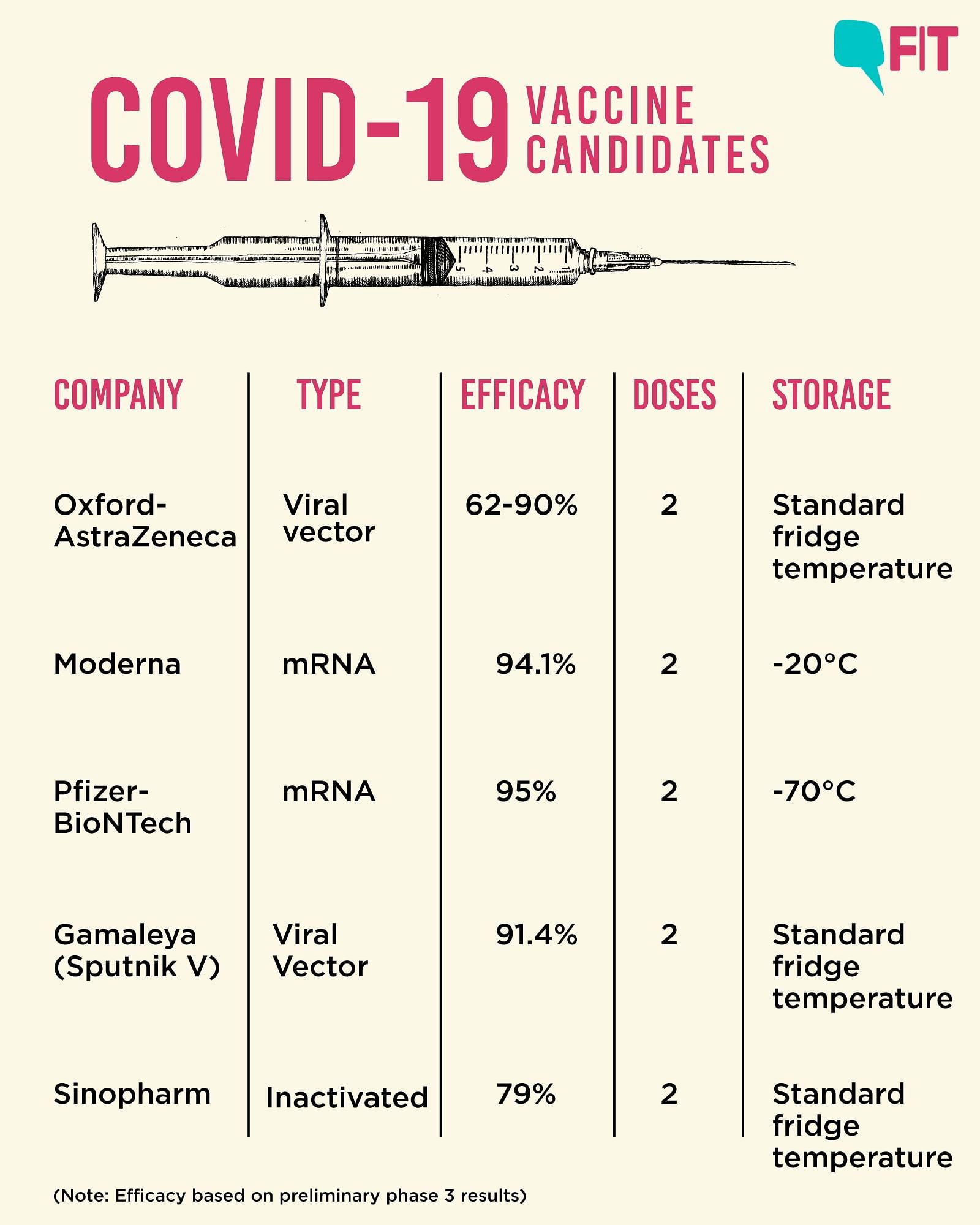
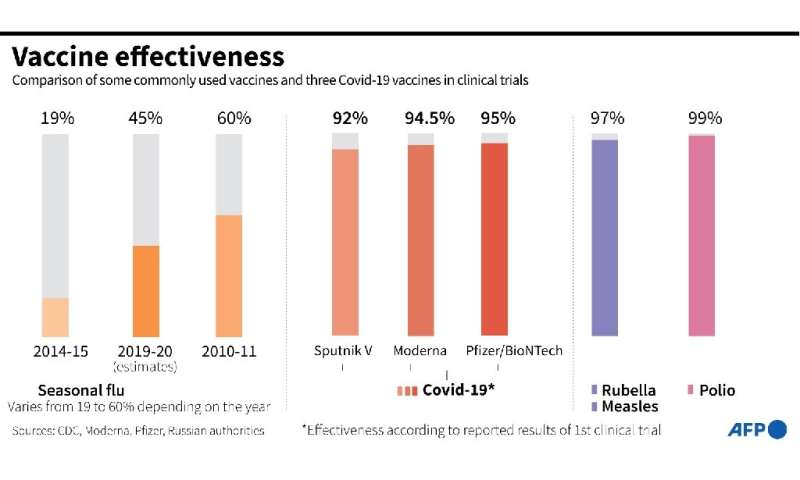
The most common adverse reactions in the clinical trial were mild to moderate injection-site pain, headache and fatigue. "Serious and severe adverse events were low in number and balanced between vaccine and placebo groups." Differences in safety profiles of vaccines must be considered in the context of efficacy. Both RNA vaccines (BNT162b2 and mRNA-1273) reported 95% and 94% vaccine efficacy, respectively (symptomatic PCR-confirmed cases were the primary clinical trial outcomes). This is substantially higher than the reported efficacy of other vaccine platforms. The efficacy of inactivated vaccines was reported as 78.1% for BBIBP-CorV and 50.7% for CoronaVac .

Efficacy of Ad26.COV2.S against moderate to severe critical Covid-19 with onset at least 14 days after administration was 66.9% . Overall efficacy of ChAdOx1-nCoV in preventing symptomatic COVID-19 across both the low dose and standard dose groups was reported as 70.4% . The efficacy of Gam-COVID-Vac, another non-replicating vector vaccine, was 91.6% . Based on the current evidence, RNA vaccines have both higher rates of adverse reactions and higher efficacy.

Due to the relative mild and transient nature of most of these reactions, RNA vaccines should be considered an excellent option to protect against COVID-19, especially in the absence of other viable candidates with similar efficacy. In addition to safety and efficacy, vaccine candidates must also be assessed in the context of the risk of disease, to determine whether each vaccine supports a favorable benefit-risk ratio or not. Such a determination is undoubtedly more important than comparing safety and efficacy between vaccine candidates as long as vaccine supply is limited and disease is prevalent. The point estimates of vaccine efficacy at these two time points across a variety of age groups are similar to the overall estimate, including among study participants ≥65 years of age who comprised approximately 20% of the study population. Point estimates of vaccine efficacy at 14 days post-vaccination are comparable in study participants with and without one or more comorbidities. In contrast, the point estimate of efficacy in participants with comorbidities is somewhat lower at 28 days post-vaccination.

Efficacy for Janssen vaccine was based on clinical trials that were conducted in countries with widely circulating VOCs , which may have impacted its overall efficacy. This is in contrast to the clinical trials for other authorized COVID-19 vaccines. Pain at the injection site is very common after administration of the currently authorized, COVID-19 vaccine. Localized axillary swelling and tenderness was a solicited adverse event in the Moderna COVID-19 clinical trial and was very common after administration with that vaccine. Local adverse events are usually mild or moderate and resolve within a few days of vaccination.

For the authorized mRNA COVID-19 vaccines, pain at the injection site was slightly more frequent in younger authorized age groups including adolescents years of age (Pfizer-BioNTech COVID-19 vaccine) compared to older adults. For AstraZeneca COVID-19 vaccine, local reactions were milder and reported less frequently after the second vaccine dose in all age groups. Similar frequencies of local reactions were reported across age groups after administration of the Janssen vaccine. Rare cases of serious blood clots, including cerebral venous sinus thrombosis, associated with thrombocytopenia have been reported in Canada and globally following post-licensure use of AstraZeneca COVID-19 vaccine.

Cases have usually occurred between 4 and 28 days after receipt of vaccine. This adverse event is being referred to as Vaccine-Induced Immune Thrombotic Thrombocytopenia . The mechanism of action is similar to heparin-induced thrombocytopenia . The exact mechanism by which the viral vector COVID-19 vaccines may trigger VITT is still under investigation. At this time, no other predisposing factors have consistently been identified in patients who develop VITT.

The rate of this adverse event is still to be confirmed, but had been most commonly estimated to be between 1 in 26,000 persons and 100,000 persons vaccinated with a first dose of AstraZeneca COVID-19 vaccine although this continues to evolve and may increase. Based on available evidence as of June 1, 2021, PHAC has estimated the rate of VITT in Canada to be 1 in 73,000 doses administered. However, as investigations continue, this rate could be as high as 1 in 50,000 persons vaccinated with the AstraZeneca/COVISHIELD COVID-19 vaccine. Additional information is currently being gathered to characterize the rate of VITT more accurately.
Based on available information, the case fatality of VITT typically ranges between 20 and 50%. Case fatality may vary with increased awareness of the adverse event and appropriate early treatment. It is unclear to what extent pre-existing immunity to any adenovirus-based vaccine vector exists in the Canadian population and what impact that could have on adenovirus based vaccine safety and efficacy.

It is also unclear as to what extent immunization with adenovirus-based vaccines elicits anti-vector immune responses and what impact that could have on homologous or heterologous booster doses with adenovirus-based vaccines. Evidence for a viral vector vaccine based on human adenovirus 5 indicated that vaccine recipients with high pre-existing immunity to the adenovirus vector had lower anti-SARS-CoV-2 immune responsesFootnote 151. The AstraZeneca COVID-19 vaccine uses a modified chimpanzee adenovirus vector . AstraZeneca found no correlation between anti-ChAd neutralizing antibody responses and anti-SARS-CoV-2 immune responses. It also found that neutralizing antibody levels were not boosted after the second dose.
However, neutralization is not the only anti-vector immune response that could impact vaccine-induced immunity. It remains unclear if immune responses to the ChAd vector will impact the efficacy or effectiveness of this vaccine. Fatigue, headache, muscle pain, chills, and joint pain are all either common or very common after the administration of the currently authorized, COVID-19 vaccines. Fever was very common after administration of the second dose of the mRNA COVID-19 vaccines and common after any dose of viral vector COVID-19 vaccines.

More than a quarter of vaccine recipients experienced headache, and/or fatigue after any dose. For the mRNA COVID-19 vaccines, systemic adverse events are usually mild or moderate intensity and resolve within a few days of vaccination. Systemic reactions are more frequent after the second vaccine dose and in younger authorized age groups including adolescents years of age (Pfizer-BioNTech COVID-19 vaccine). For AstraZeneca COVID-19 vaccine, systemic reactions are milder and reported less frequently after the second vaccine as compared with the first in all age groups.

The frequencies of systemic reactions that were reported after administration of the Janssen vaccine were similar across age groups. The pooled rates of local and systemic reactions were significantly different between vaccine platforms. Inactivated vaccines, protein subunit vaccines, and DNA vaccines had lower rates of local and systemic reactions compared to RNA vaccines, non-replicating vector vaccines, and virus-like particle vaccines. The safety profiles of BNT162b2, mRNA-1273, ChAdOx1-nCoV, Ad26.COV2.S, and CoronaVac were relatively benign in the elderly, and both the frequency and the intensity of local and systemic reactions decreased with age. The rates of SAE, including non-fatal serious AEFI and death, were similar in vaccine and placebo groups in clinical trials.
Reporting rates of common AEFI after mass public vaccination were lower than in clinical trials. Several unexpected rare adverse events, which resulted in severe outcomes, have been noted in post-authorization surveillance. Evidence for a COVID-19 viral vector vaccine based on human adenovirus 5 indicated that vaccine recipients with high pre-existing immunity to the adenovirus vector had lower anti-SARS-CoV-2 immune responsesFootnote 151. Janssen found no correlation between anti-Ad26 neutralizing antibody responses and anti-SARS-CoV-2 immune responses. It remains unclear if immune responses to the Ad26 vector will impact the efficacy or effectiveness of this vaccine.
The efficacy and effectiveness of COVID-19 vaccines in immunosuppressed populations is currently unknown, but evidence of a diminished immune response is emerging. Study participants showed diminished or delayed immune responses to mRNA or AstraZeneca COVID-19 vaccines. The type of immunosuppressive therapy or condition affected the immune response to COVID-19 vaccines, leading to a lack of humoral and cellular responses in some cases or diminished levels in those who did develop responses compared to healthy controls. Given the limited number of participants and the lack of an immunological correlate of protection against SARS-CoV-2 infection, there are limitations in interpreting the significance of these results. Evidence on the safety of vaccine booster doses is available from observationalFootnote 25 and clinical studiesFootnote 26 Footnote 27 Footnote 28.

Occurrence of solicited and unsolicited systemic adverse events in individuals with prior SARS-CoV-2 infection was slightly higher compared to the SARS-CoV-2 naïve population, primarily in younger adults. However, there was no observed increase in the frequency of more severe adverse events in this population. Two observational studies included less than 100 patients with persistent symptoms from prior COVID-19 infections . In this subgroup, receipt of COVID-19 vaccination with either an mRNA or viral vector vaccine was not associated with a worsening of long COVID symptoms or increased reactogenicity following immunization.

The onset of new autoimmune disease or disease exacerbation following vaccination with mRNA COVID-19 vaccines was rare or comparable to the background incidence of these events in the general population. Safety data in these populations following vaccination with a viral vector vaccine is not available. Combined evidence from clinical trial and observational study data available to date have shown that the AstraZeneca COVID-19 vaccine offers protection against symptomatic COVID-19 disease and hospitalization in adults ≥18 years of age after receiving at least one dose. Clinical trial data available to date have shown that the AstraZeneca COVID-19 vaccine has demonstrated moderate efficacy against symptomatic, confirmed COVID-19 of approximately 62% in those years of age. Efficacy of a two-dose series increased to approximately 82% when the interval between doses was 12 weeks or more.
In adults 65 years of age and over, observational data from the UK of vaccine effectiveness after one dose have shown a reduction in the risk of symptomatic disease and hospitalization. Evidence on the safety of COVID-19 vaccination in these individuals is emerging. The frequency and severity of adverse events following vaccination with an mRNA COVID-19 vaccine in these populations were comparable to that of non-immunosuppressed individuals in these studies and what was reported in clinical trials. Evidence on the safety of COVID-19 vaccination of individuals with prior SARS-CoV-2 infection is available from observationalFootnote 25Footnote 51Footnote 52 and clinical studiesFootnote 26Footnote 27Footnote 28.

The occurrence of solicited and unsolicited systemic adverse events after the first or second dose in individuals with prior SARS-CoV-2 infection was slightly higher compared to the SARS-CoV-2 naïve population. Side effects observed during the clinical trials were typically mild, commonly reported side effects of vaccines and do not pose a risk to health. Safety data in this population following vaccination with a viral vector vaccine is not available. Exploratory analyses for the AstraZeneca viral vector vaccine has not demonstrated efficacy against confirmed SARS-CoV-2 asymptomatic infection, however the number of asymptomatic infections was small.

The clinical trial of the Janssen COVID-19 vaccine found the vaccine to have moderate protection against asymptomatic and undetected COVID-19 infection. Vaccinated people are less likely to develop symptomatic infection based on evidence from trials and other studies. In such cases a single dose of either vaccine , reduces the risk of transmission from cases to their household by 38-49% compared to unvaccinated individuals. Furthermore, age of the case or contact was found to have limited impact on these findings. This real world study provides further evidence that vaccines may not just prevent infection but may also prevent transmission in cases of vaccine breakthrough. This large community-based survey of randomly selected households across the UK examined vaccine effectiveness against the COVID-19 Delta variant in those aged 18 years and older.

This study found that the effectiveness of the Pfizer-BioNTech and Oxford-AstraZeneca vaccines is reduced with the Delta variant. Two doses of the Pfizer-BioNTech or Oxford-AstraZeneca vaccine provided the same protection as having previous infection. Those who were vaccinated after infection had more protection than those vaccinated without having had prior infection. Protection was higher among younger age groups and the time between vaccine doses did not affect effectiveness. Compared to Oxford-AstraZeneca vaccines, the Pfizer-BioNTech vaccine has greater initial effectiveness but this declines faster than Oxford-AstraZeneca. A single dose of the Moderna vaccine had similar or greater effectiveness compared to a single dose of the Pfizer-BioNTech or Oxford-AstraZeneca vaccines.

For those who were infected with the Delta variant after vaccination, peak levels of virus were similar to those in unvaccinated individuals. Overall, this study found that obtaining two vaccine doses is the most effective way to ensure protection against the COVID-19 Delta variant, however vaccine effectiveness is reduced and peak viral load is higher with the Delta variant. Current evidence about the safety of COVID-19 vaccines relies mainly on data from phase 1–3 randomized controlled trials and vaccine safety surveillance system in several countries. We found three reviews of the safety of COVID-19 vaccines , which combined study experimental groups, and did not examine the heterogeneity between vaccine platforms and participant age groups. Here, we conduct a rapid review and meta-analysis to summarize the safety data of COVID-19 vaccine candidates. We aim to comprehensively evaluate the rate of solicited, unsolicited, and serious AEFI in each clinical trial and to estimate the relative risk of AEFI by vaccine platform and participant age group.

We also collected post-authorization surveillance data from around the world to look for uncommon and delayed onset reactions. This overview of the safety profile of COVID-19 vaccines will support responses to potential safety issues and inform decision-makers evaluating vaccination strategies around the globe. The outbreak of the COVID-19 epidemic has promoted the rapid development of the vaccine industry. In just one year, more than one hundred COVID-19 vaccines from various platforms have entered clinical trials, which has laid the foundation for the research and application of sequential immunization strategies. The COVID-19 vaccines of different platforms have different immunological characteristics.

The use of heterologous vaccines for sequential immunization can theoretically avoid boosting immunization of non-target proteins and enhance the strength of the immune response against the target antigen. Among the various vaccines currently being researched and marketed, some vaccines are mainly used to induce T cell responses, and some are mainly used to induce antibody responses. By using vaccines with different immune characteristics for sequential immunization, it is possible to obtain higher levels of antibody response and T cell response. In addition, sequential immunization may theoretically reduce the risk of ARs caused by a second dose of a single vaccine.
In particular, reports have shown that the incidence of ARs increase when the second dose of mRNA vaccine is administered . However, it should be noted that the US CDC has clearly pointed out that the safety and effectiveness of mixed vaccination of different types of vaccines have not been verified, and mixed vaccination is currently not permitted, except under special circumstances. Although availability of vaccines from different platforms makes a compelling case for sequential immunization strategies, further studies are required to ascertain the benefits of such a strategy for COVID-19. Safety evidence is based on interim analyses of 23,745 participants of which 12,021 received at least one dose of the AZ COVID-19 vaccine and 11,724 received a control. Solicited adverse events occurring within 7 days after any dose were assessed among 2648 vaccine recipients who received at least one dose and 2497 control recipients. Approximately one third of study participants received their second vaccine dose within 6 weeks of receiving Dose 1.

The majority (~90%) of study participants in the safety cohort were less than 65 years of age. The median duration of follow-up was 105 days post-Dose 1 and 62 days post-Dose 2. In a subgroup analysis in study participants who received the SD/SD vaccine regimen, vaccine efficacy against confirmed COVID-19 cases occurring at ≥15 days after dose 2 was estimated by dosing interval and age group. These ad-hoc subgroup analyses were performed in participants years of age from the COV002 clinical trial and in all study participants who received the SD/SD regimen , dichotomized into groups years and ≥65 years of age.

The clinical trial data demonstrates that the authorized mRNA COVID-19 vaccines are efficacious over the short-term in individuals with or without evidence of prior SARS-CoV-2 infection. The efficacy of the Janssen COVID-19 vaccine in those with evidence of prior infection is inconclusive at this time due to small sample size, and this outcome has not been assessed for AstraZeneca COVID-19 vaccine. Clinical trial data show that efficacy increased as the interval between doses increased. At present, there are insufficient clinical trial data in adults ≥65 years of age to assess vaccine is efficacy in this age group.